
Nerfing the Abstract #2
Nerfing the Abstract #2
It’s not a new phenomenon


While Covid certainly brought many more welcomed and scrupulous eyes to the sausage making of Science, the shenanigans are not superannuated.
The cannabis field has been suffering from Fiat science since prohibition. While it’s illegal to research independently, you can sign up for a hard to acquire DEA license and some NIDA funding if you sing the right prohibitionist songs. Although keep in mind that some labs that attempt to take this legitimized approach get raided by the DEA when they apply for a license.
https://www.cannabisculture.com/content/2010/02/15/medical-marijuana-lab-latest-be-raided-dea/
Such songs will likely entrap shock jocks like Alex Berenson to cling to results that support his book sales but if a paper of this quality was in support of Ivermectin use, he would rightfully pillory it.
Here is more Lancet lunacy.
It’s a correlation/causation meta analysis paper that suffers in many regards.
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(22)00161-4/fulltext
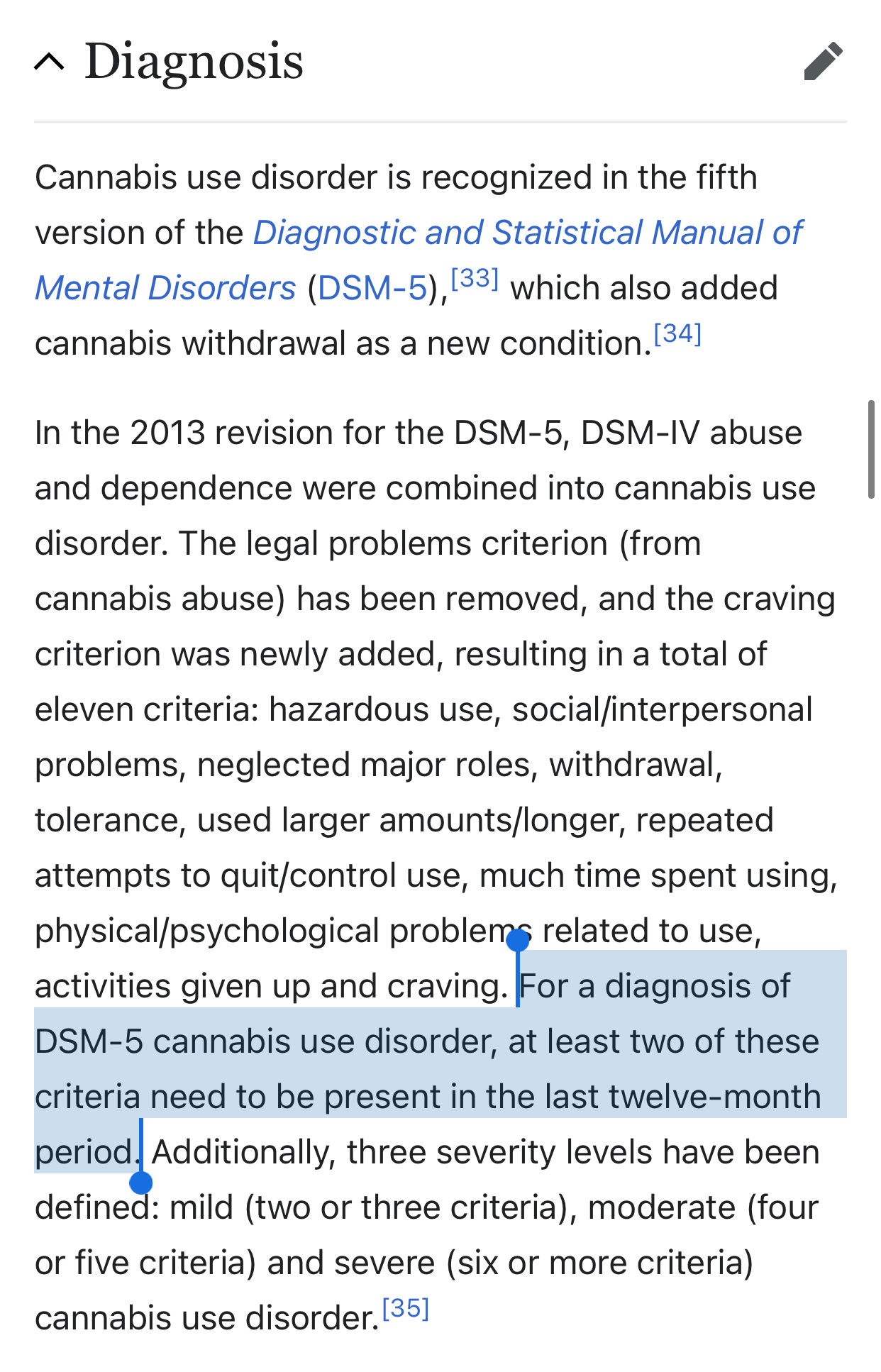
First critique is that the paper sanctifies the Cannabis Use Disorder or CUD fraud.
If you believe this disease exists, you should work on water use disorder next. It’s literally a disease that simply classifies people who use frequently as a disorder. People who take SSRIs daily, never get classified with such a disorder. It ignores medical cannabis use may require daily use and this isn’t a disorder but an action taken to to correct for something else.
Note the diagnosis is a choose your own adventure of “any 2 criteria” and any daily medical user would be labeled with this.
This is not to say that some people don’t have a cannabis consumption problem but the diagnosis is intentionally broad and lacks nuance.
Second issue with CUD is that it’s scientifically illiterate. It is meant to describe high THC Use Disorder but fails to understand that high CBD, CBG, CBDV, THCV cultivars exist in the market place and have completely different pharmacology than THC. In fact, CBD is a contender for rectifying cocaine based CUD (cocaine use disorder) and also championed for cannabis use disorder (see clinical trial below). So some cannabis use can be used to curtail other cannabis use.
Capisce?
https://pubmed.ncbi.nlm.nih.gov/33464660/
https://pubmed.ncbi.nlm.nih.gov/32735782/
But prohibitionists love to throw the baby out with the bath water and conflate this whole topic usually under the even less descriptive term ‘marijuana’.
So let’s look at the language in the lancet study and then revel in how quickly these researchers want their work converted into policy despite their weak associative finding.
That’s an accurate assessment of all of Alex Berensons drivel on the topic and likely what some reviewers demanded be stated in this paper.
Now let’s look at how quickly these researchers want the government guns tuned to their unfounded suggestions..
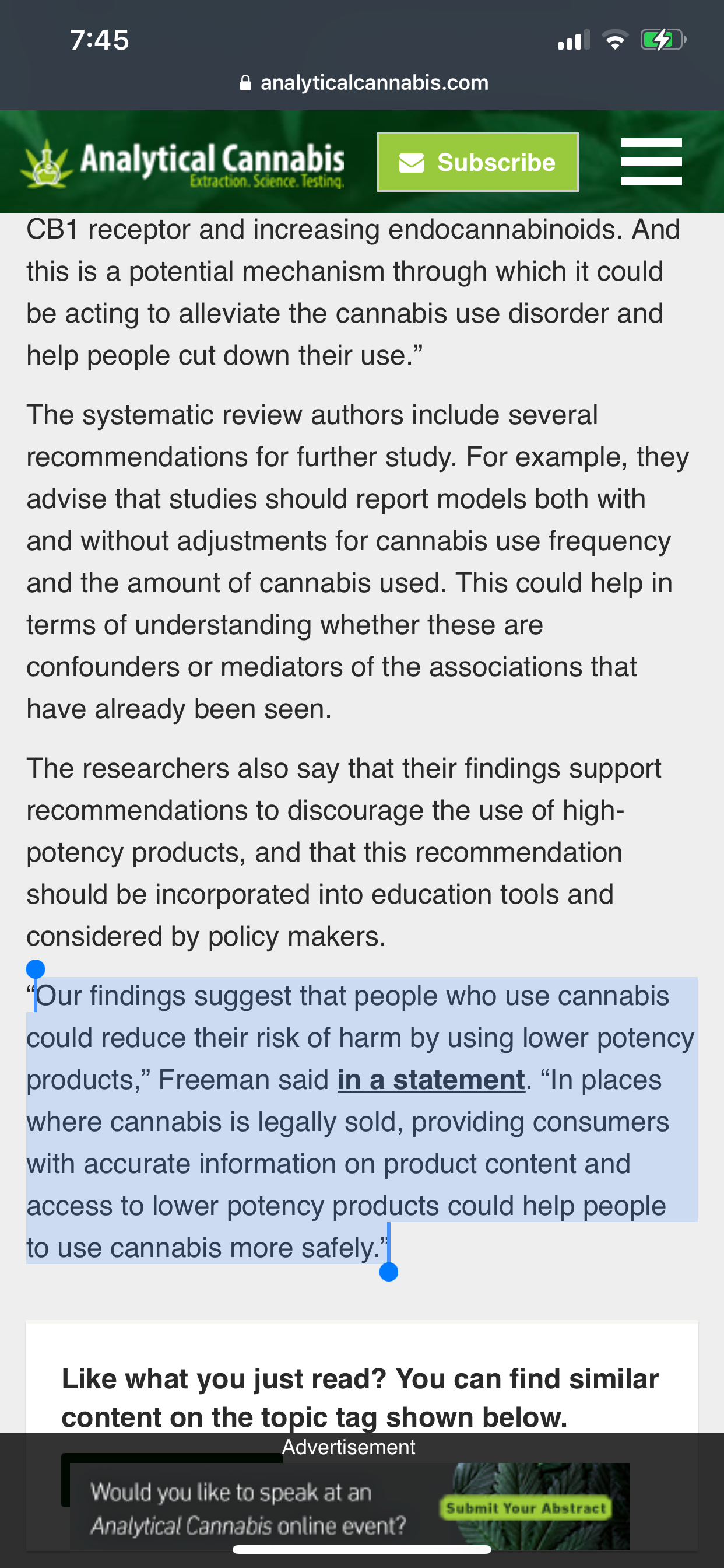
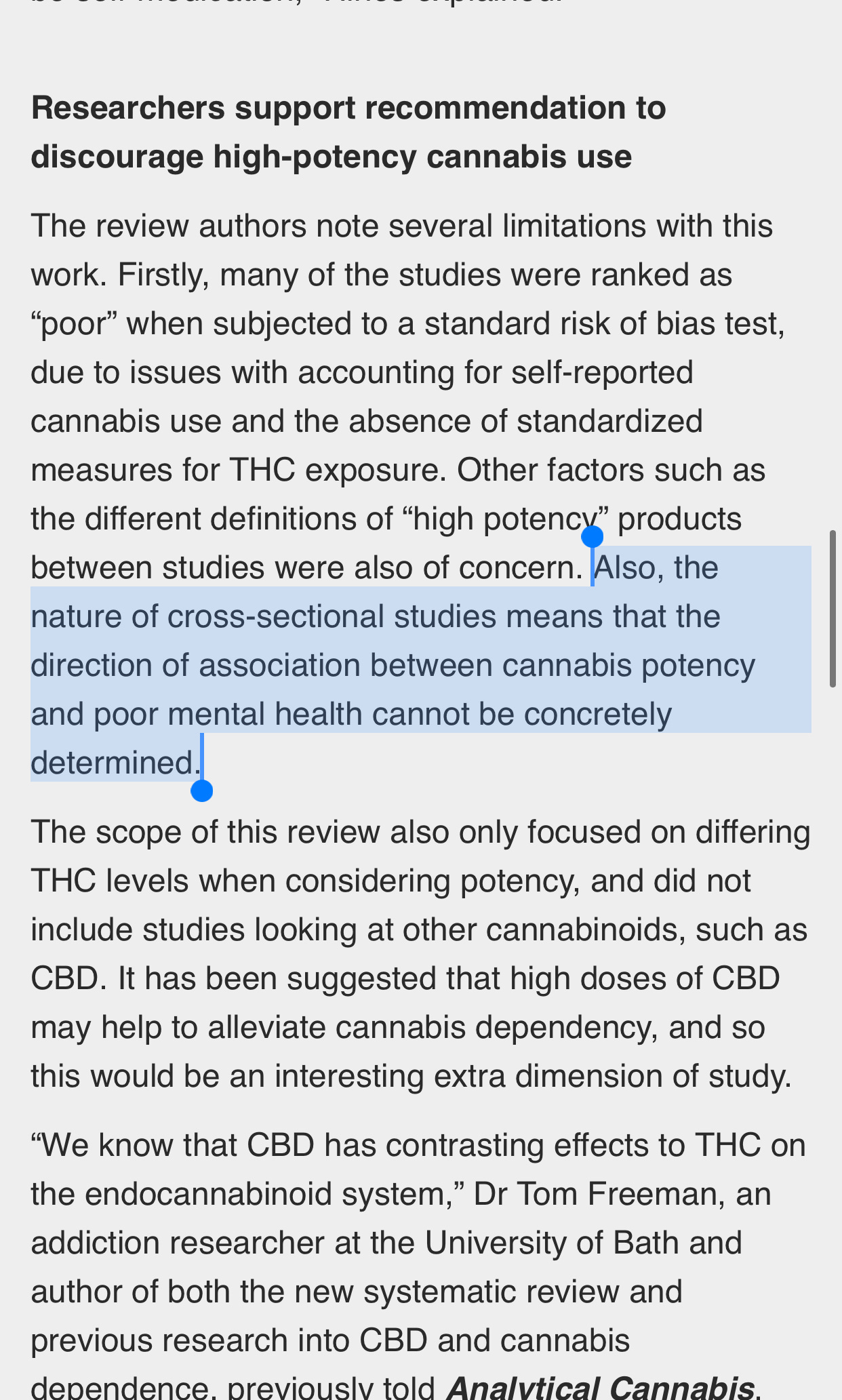
Straight from association with multiple confounders to bans/discouragement on high potency products.
Never even a mention of the fact that people will just consume more of the low potency product to obtain their desired result and that requires more smoking risks to reach desired dosage.
It’s as if you banned only whiskey but allowed wine and believed that would curtail alcoholism. More calories are required to reach desired dose with lower potency products.
This is what passes for Lancet level Cannabis science. If it’s in vogue and sings the NIDA songs, it publishes regardless of the associative nature or confounding variables.
Nerfing the Abstract isn’t new to C-19. It’s the signature of government funded science.
I was tentatively “diagnosed” with Cannabinoid Hyperemesis Syndrome a few weeks ago after I went to the ED due to persistent vomiting/nausea. My drug screen came back positive so there’s clearly no other reason for these symptoms 😂. Is this anything like CUD?