

Open Letter to Dr. Lisa Kerr
Your letter has been retracted


The following letter was sent to the Primer Minister of Australia. It evoked a response from Dr. Lisa Kerr from the Laboratories Branch of Medical Devices and Product Quality. There are many errors and short comings in Dr. Kerr’s letter which I will address below.
The Russell Broadbent letter is below for your reference.
-END OF BROADBENT LETTER
Here is Dr. Kerr’s Response. I’ve also included it towards the end of this thread.
This gets a “Pants on Fire” rating by Scientists more versed in this topic than her. Note, I cannot find Dr. Lisa Kerr’s google scholar record. If anyone finds it, please post it in the comments but from the nature of her comments on this topic, she is way over her skis responding to this topic. This is very odd as you will see she relies on many appeal to authority arguments in her letter yet she has none herself.

Let dissect her letter.
The 3rd paragraph speaks to expired vaccine vials. This is evidence that Dr. Kerr is not reading the references supplied to the Prime Minister. She is parroting fact checkers who have no commitment to accuracy.
The very first paper that described this problem (McKernan et al) used both expired and non-expired vials.
This argument always backfires on fact checkers once you provide evidence that Expired vials were given to patients!
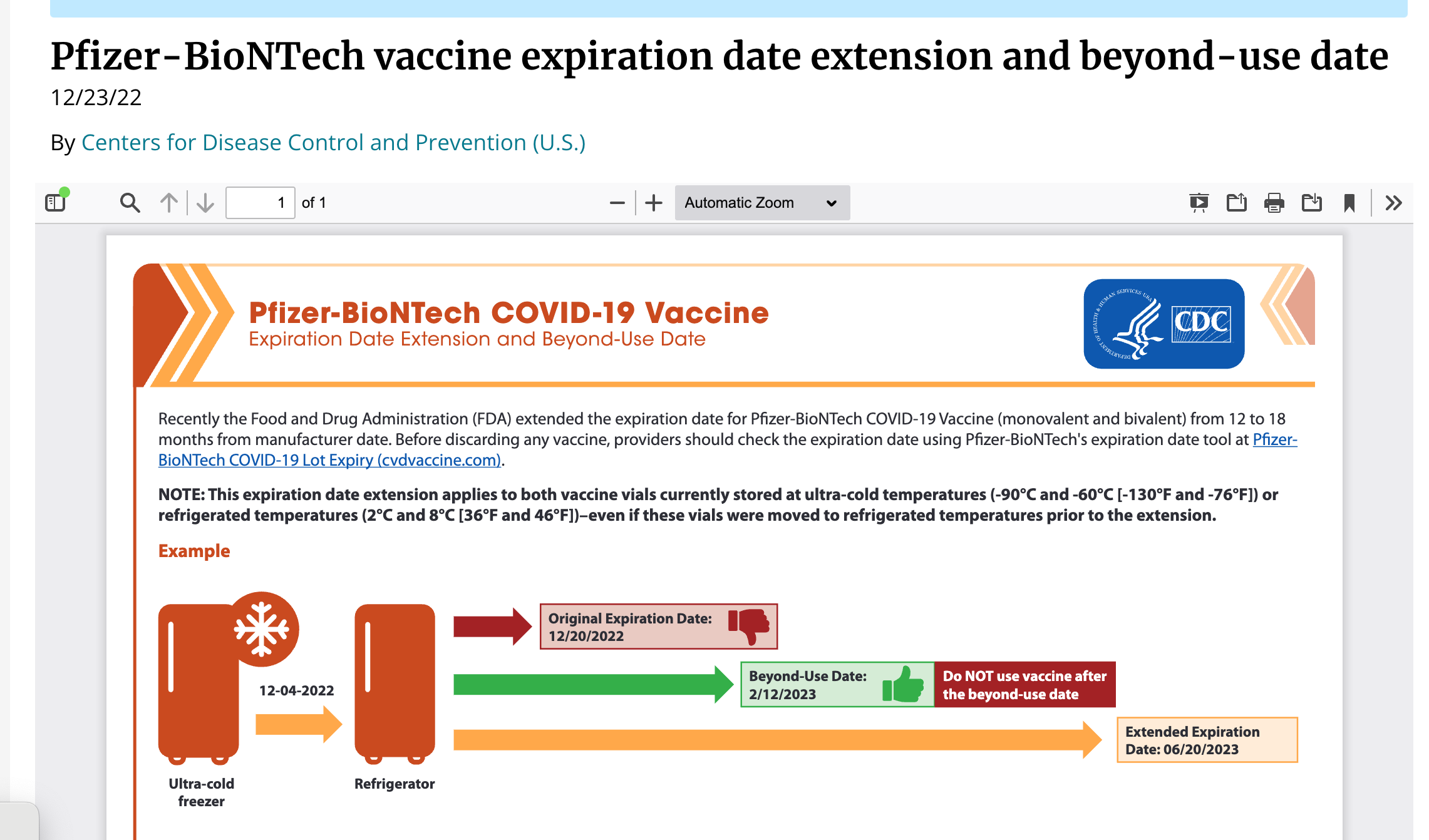
Multiple times regulatory agencies extended the expiration dates of vials via Fiat declaration with no additional clinical trial!
Anyone versed in DNA knows that expiration of vials does not magically replicate DNA. If anything it would decay the DNA and make the measurements more in Dr. Kerr/Pharma’s favor. RNA is less stable than DNA, so the expiration dates are more of a concern for RNA. DNA can be retrieved from ancient mammals. The 1.2 million year old Woolly Mammoth genome is the best example of this.
Opening with such an easily refutable argument would imply Dr. Kerr is not fit for this role and is performing a very superficial analysis.
Dr. Kerr goes on to condemn ‘unvalidated methods’ while her methods remain behind redactions. There is no such thing as a ‘validated protocol’ that remains closed to inspection.
She continues to condemn our laboratories as being ‘unaccredited’ but will not share the accreditations of the labs that performed her testing. Very recently the FDA published a paper confirming our work. Is she suggesting the FDA is non-accredited?

This is an appeal to authority fallacy, only she refuses to share who her authority actually is and what their methods are.
Having been the Team Leader for Research and Development on the Human Genome Project at Whitehead/MIT with over 57,000 citations to my work in the field of genomics, I find Dr. Kerrs arguments fallacious and elitist. This is not a time for appeal to authority arguments but since Dr. Kerr has put this argument forward let me respond to it.
I have 28 years of experience in this field and even invented novel methods for DNA sequencing (SOLiD Sequencing) and DNA purification (SPRI). These projects resulted in successful patents and companies that were acquired by the most prestigious genomic companies in the field (Beckman Coulter and Applied Biosystems). The SPRI based DNA purification procedures I invented and developed with a ~100 person company I founded, are used in over 80% of the next generation sequencing methods in the market today. James Watson (the discoverer of the structure of DNA) has written about my success in his book and I’ve been invited to the White House and the House of Lords for my contributions to this field. This cannot be said for Dr. Kerr and any of the anonymous experts she appeals to. These appeals to authority do not address the evidence we have provided and are a desperate sign of poor argumentation from an agency that has over 95% of its funding delivered from the manufacturers we are critiquing.
Dr. Kerr claims their methods have been vetted by hundreds of experts in the field, yet Dr. Kerr will not list them. We have no reason to believe this unsupported statement because the methods that have leaked from the TGA demonstrate they are irresponsible methods that would never pass peer review.
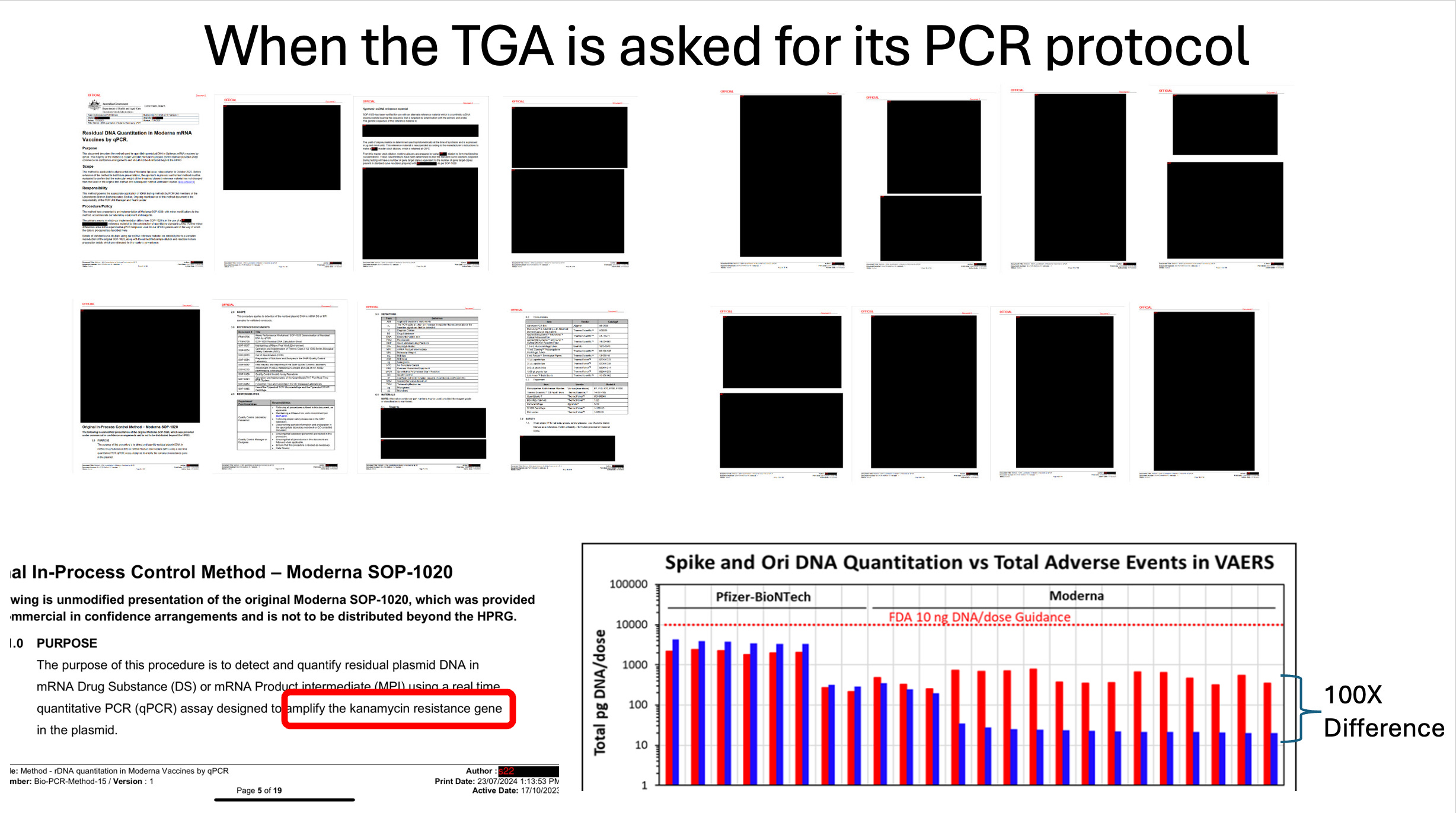
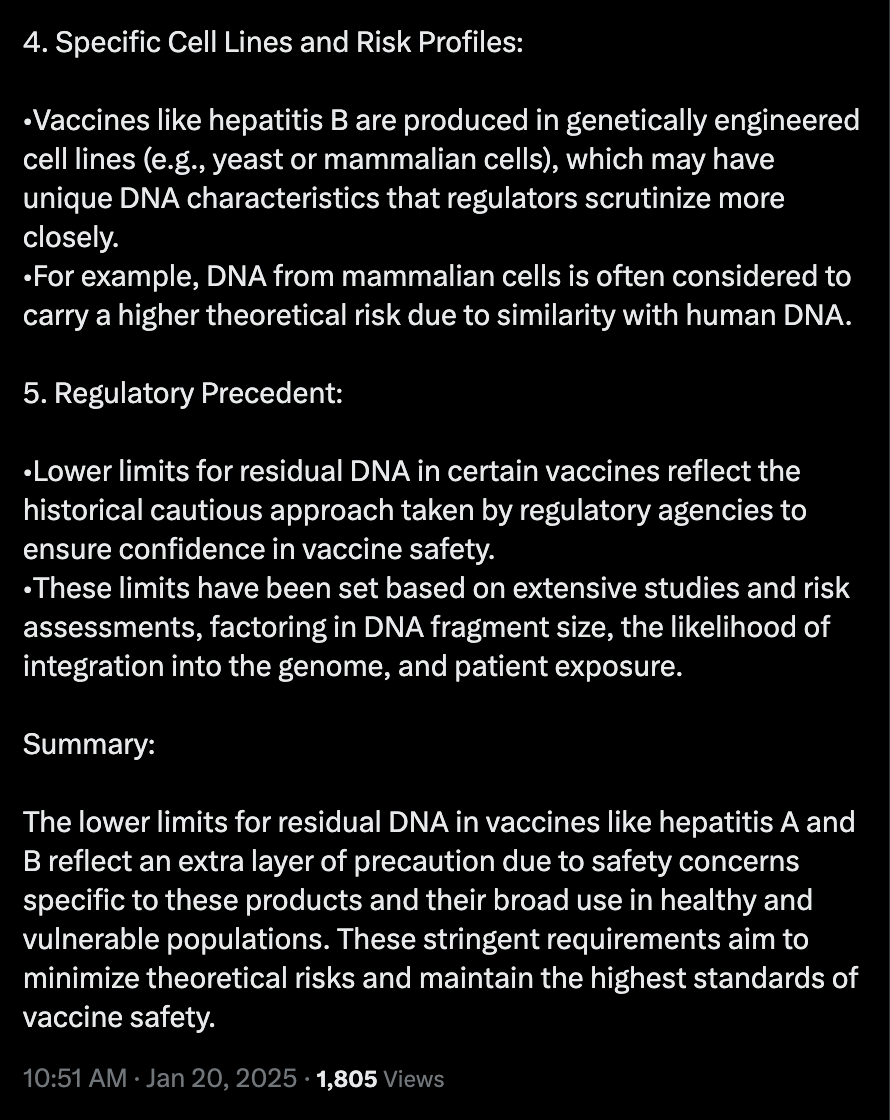
It is very clear from the methods FOIA’d from the TGA that they are using a qPCR method with a single amplicon and no internal control. This is a violation of MIQE guidelines (See ChatGPT below). Every C19 qPCR assay used multiple qPCR amplicons to assess the presence of the virus. This is why we do not believe you have 100 secret experts as none of them would agree with this egregious violation of industry standards.
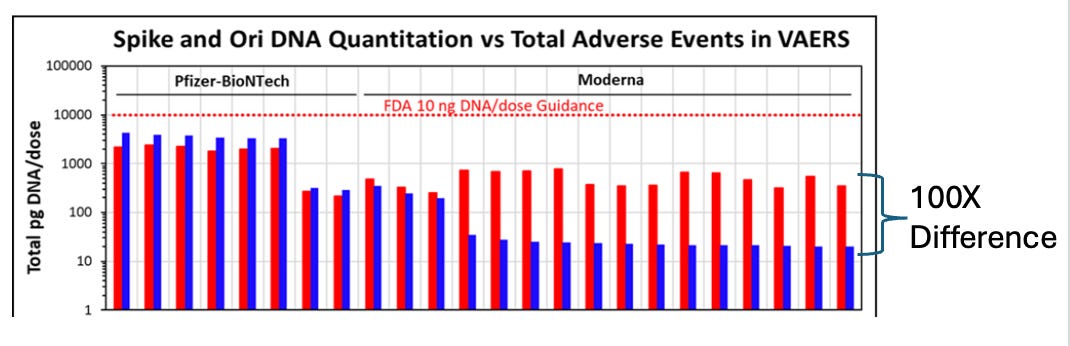
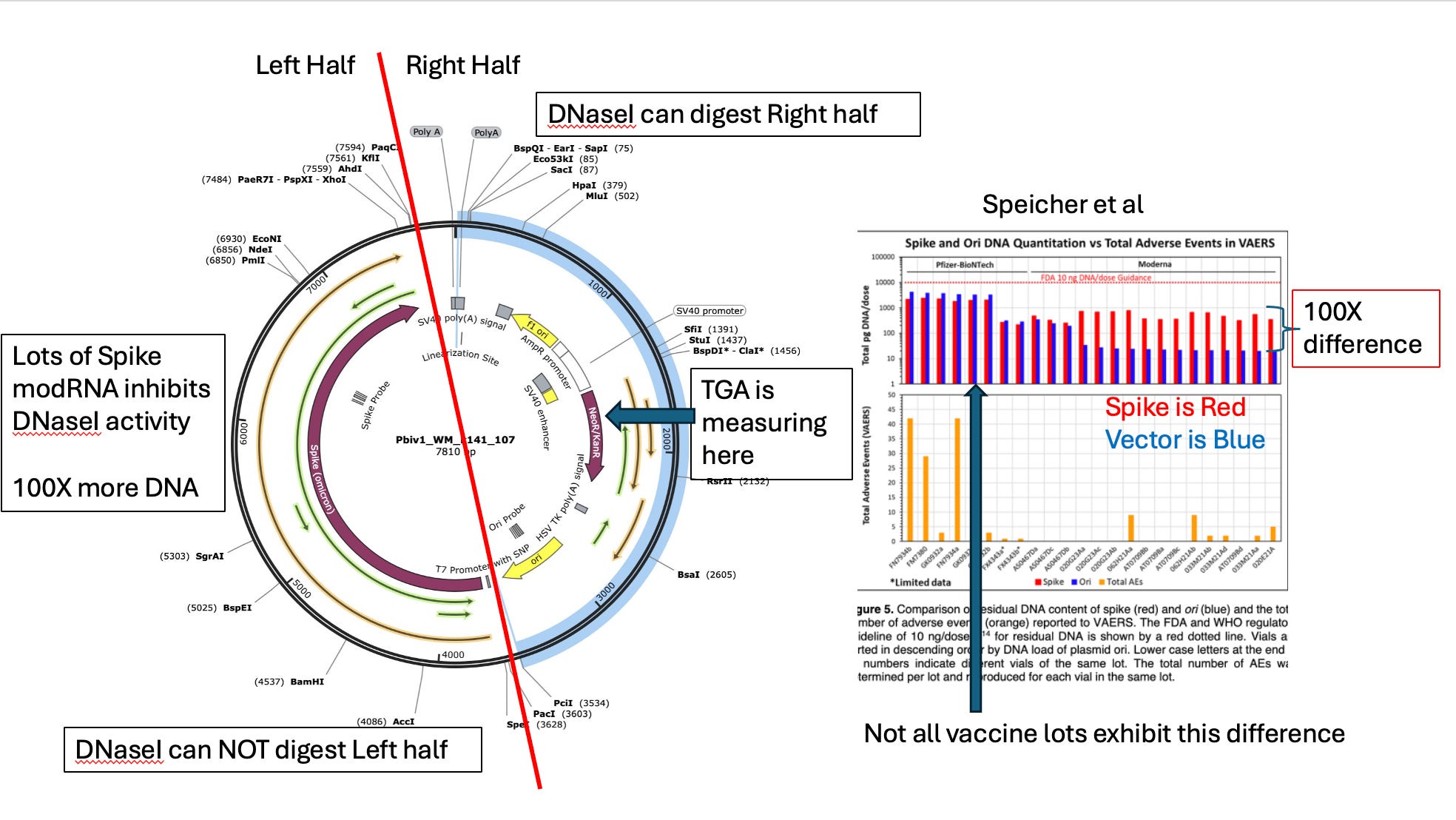
Speicher et al also demonstrated that the use of 2 qPCR amplicons manifests in 100 fold difference in quantitation of DNA from these vaccines.
Why would this occur?
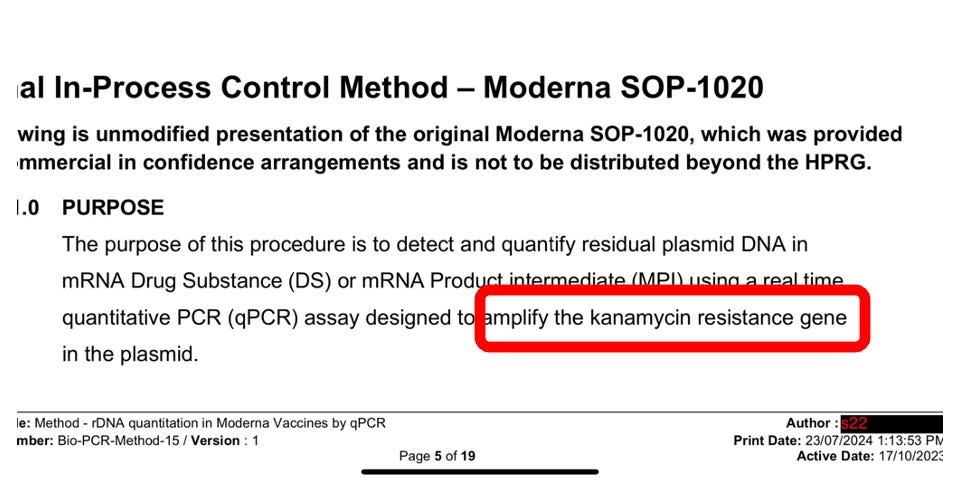
The DNA encoding the spike protein has modRNA bound to it that inhibits the DNAseI from processing and removing this DNA (Sutton et al). The TGA assay (Kan gene) doesn’t look at the spike region of the plasmid. This is why Dr. Kerr/TGA are 100 fold off in their estimates.
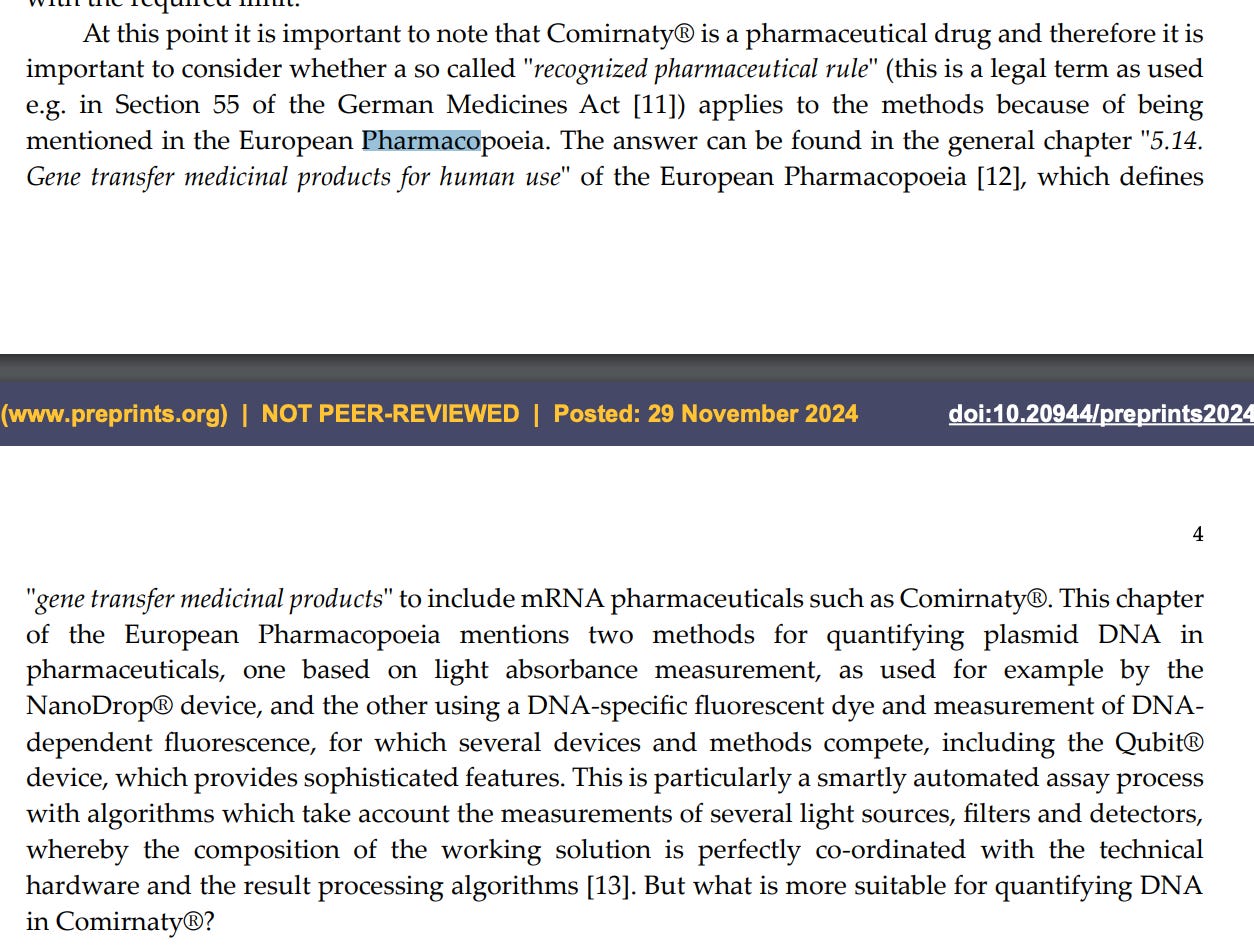
Your methods are not published in the Pharmacopeia. Please provide us with the exact method that includes primer sequences, and qPCR conditions that can be replicated by another laboratory. Declaring something is ‘validated’ while hiding these key methods is fraud. This is required transparency for any validated method. Konig et al and Konig et al will remind you that Fluorometry IS mentioned in the European Pharmacopeia for DNA quantitation.


This leads us to Page 2 of Dr. Kerr’s letter where she critiques fluorometric methods.
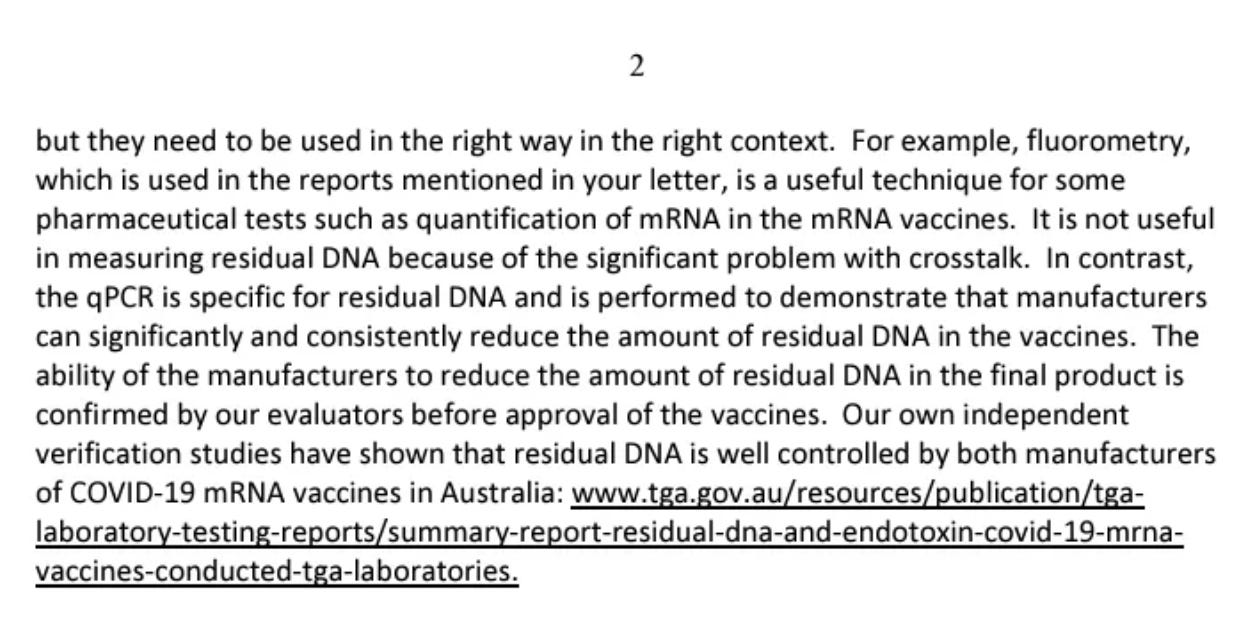
Dr. Kerr claims, without citation, that Fluorometry only has cross talk when monitoring DNA.
This is false.
Jones et al demonstrates that RiboGreen used to measure RNA actually binds DNA 2X as much making the cross talk problem more of a problem for monitoring RNA than DNA. Fluorometry is used to measure the RNA in these vials and has a larger cross talk problem than PicoGreen used to measure the DNA. Dr. Kerr has this exactly backwards and is likely parroting other unskilled fact checkers who have spread this rumor. The manufacturers (Thermo) have specs demonstrating the cross talk with PicoGreen (A DNA specific Dye) staining RNA is <10% at these concentrations.
In addition to Dr. Kerr having the crosstalk issues reversed, she has ignored the efforts of scientists to remove the RNA before using PicoGreen.
McKernan et al, Speicher et al and Kammerer et al used RNaseA to remove all RNA in the sample making Dr. Kerr’s argument moot. This RNaseA treatment does lower the DNA signal but still leaves it above the 10ng limit.
Your appeal to qPCR does not address the Moderna patents that warn how error prone this qPCR approach is. The CEO of Moderna (Stephen Bancel), the company Dr. Kerr is supposed to regulate, disagrees with Dr. Kerr’s comments. Can Dr. Kerr please address this contradiction of hers?


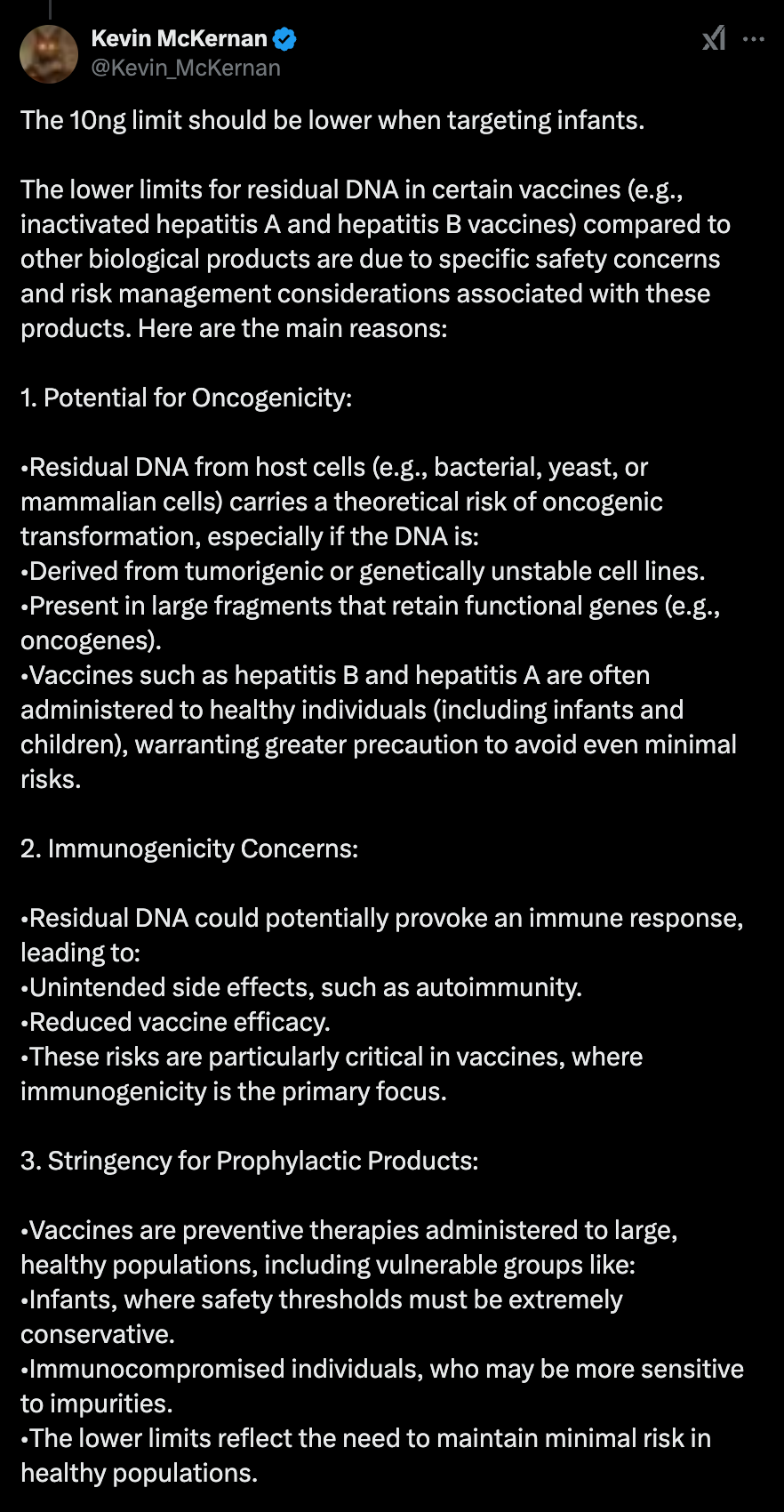
Dr Kerr then goes on to claim there is a large safety margin with 10ng of DNA.
This is false.
Vaccines for new borns have even stricter limits and are set 10-100 fold lower than 10ng specifically citing DNA integration risks. Even ChatGPT knows this, just not regulators like Dr. Kerr.
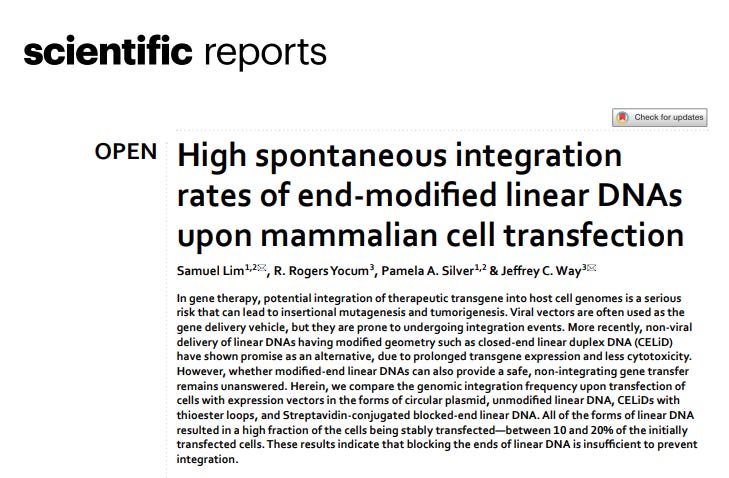
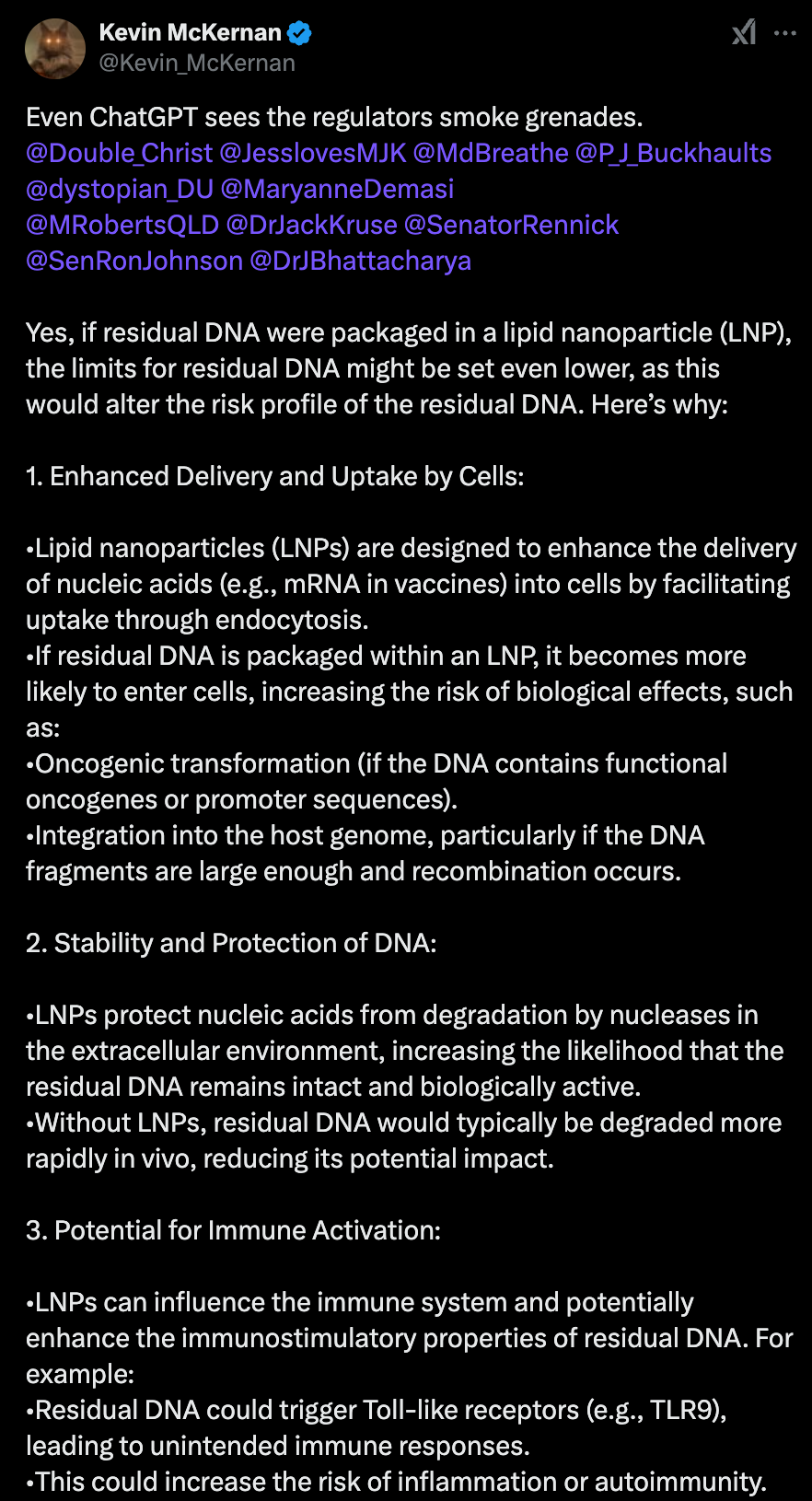
All of these 10ng studies are based on Naked DNA injection. She has not addressed the elephant in the room which is that this DNA is LNP wrapped and does not have the half life she is expecting. None of Dr. Kerr’s calculations are relevant to LNP encapsulated DNA. Once again ChatGPT confirms this as do many citations we provide such as Lim et al. Once transfection reagents are in play, the integration risks skyrocket.
Dr. Kerr then claims the DNA sequences are non-functional.
This is also false.
Drayman et al demonstrates the SV40 promoters bind to the tumor suppression gene P53. See Figure 7. There are 50-500 Billion copies of these per dose.
Dean et al demonstrates SV40 Enhancers are nuclear targeting sequences used in gene therapy
Senigl et al demonstrate the SV40 Enhancer is a somatic hypermutability element with potential tumorigenic activity.
Strayer et al- demonstrate plasmids with SV40 components but lacking the T-antigen integrate into genomes.


This sequence was never disclosed to patients and Dr. Kerr is busy running cover for her sponsors instead of correcting for this fraudulent omission.
Dr. Kerr’s final paragraphs repeat many errors regarding Fluorometry which is in fact referenced in the European Pharmacopeia while the qPCR methods you defend are recommended against in Moderna’s own patents. Likewise, the methods the TGA have disclosed are in violation of MIQE guidelines (No Internal Control) using a single amplicon in the wrong part of the plasmid. These nucleic acid based products have RNA and DNA which is self complementary in the vials. DNaseI cannot process DNA that is hybridized to RNA (Sutton et al) so the manufacturers methods are failing to digest the spike DNA while the TGA/Pharma are only looking at the Kan DNA. This has been known since 1997. Just not known by Dr. Kerr.
Fluorometry measures all DNA in solution and is not primer and probe specific and thus isn’t blind to this differential digestion from DNaseI.
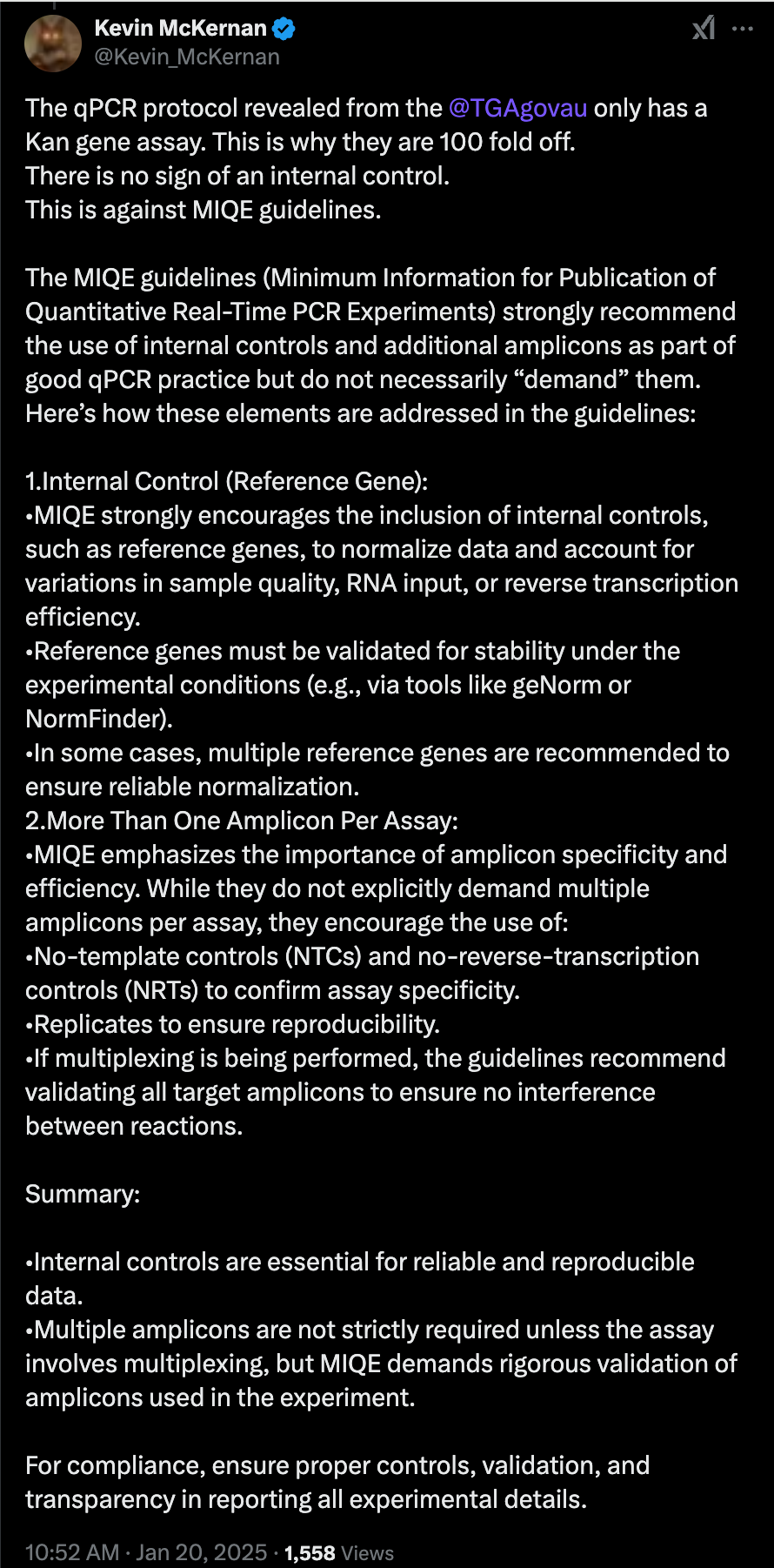
It is well known from the EMA leak that Pfizer has a qPCR assay designed for the spike region of the plasmid to confirm the sequence identity of the spike insert. Why is this qPCR amplicon NOT used to quantitate the DNA? Why are they cherry picking the broken Kan qPCR assay which the TGA will not share the primer sequences of?
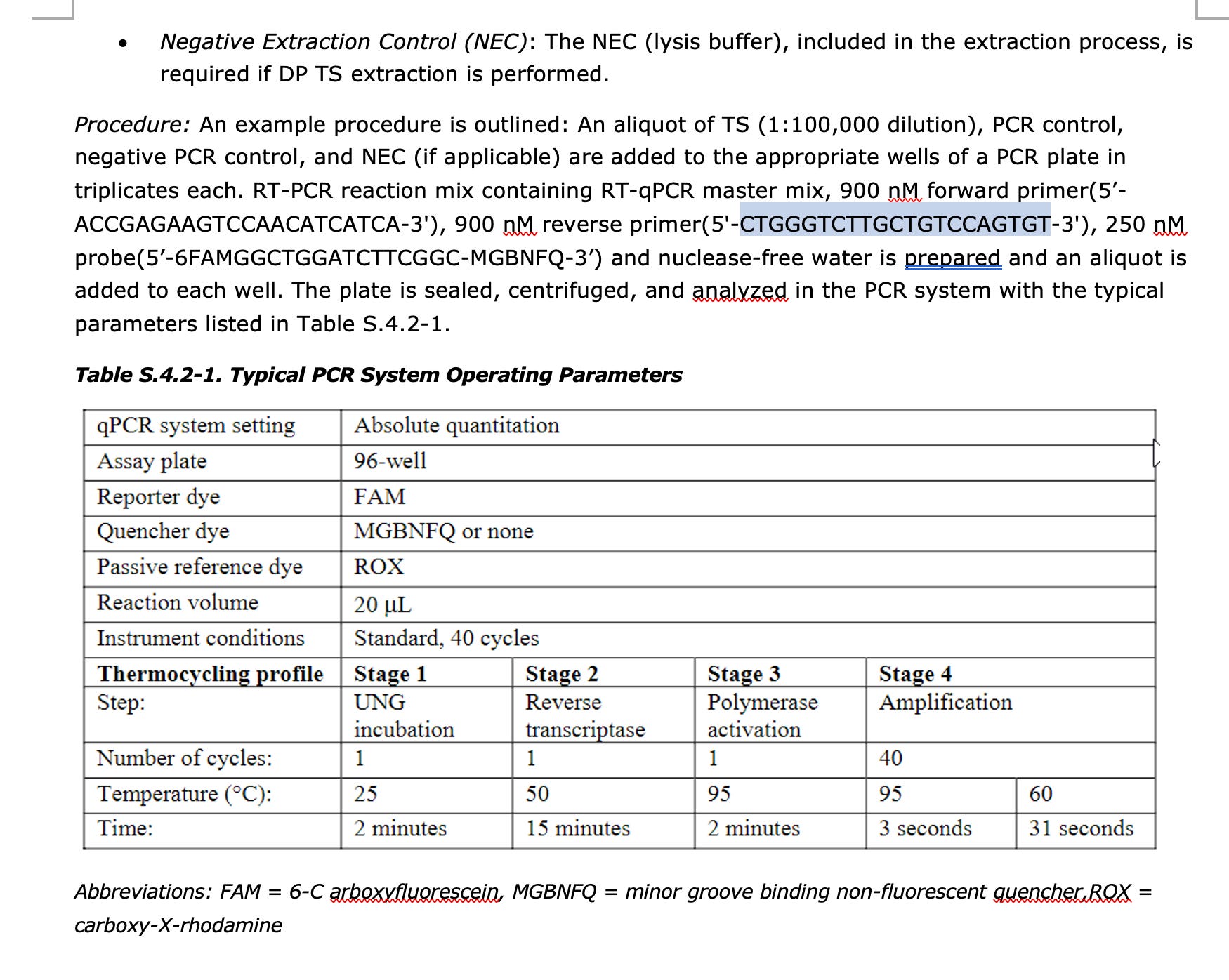
Below are RT-qPCR primer sequences that target the Spike sequence in Pfizer. These are disclosed on page 81 in the EMA documents. This demonstrates that Pfizer has a validated qPCR assay that can monitor the spike DNA but it IS NOT BEING USED to quantitate the residual DNA?
We know exactly why they are not using this spike qPCR assay, because if they did, they would see more DNA than the Kan assay predicts. Dr. Kerr’s regulatory failures have allowed this fraud to continue as she is not skilled in this field to understand this deception.
Dr. Kerr’s final paragraph asks for us to notify her of further publications on this topic. The FDA just published a paper finding 6-470X the 10ng limit of DNA (Wang et al). They also chose to use Fluorometry + RNAseA. Are these also unvalidated scientists and labs? Why is all of the peer reviewed literature resorting to Fluorometry but your secret panel of experts is using a broken qPCR assay that Moderna teaches against?
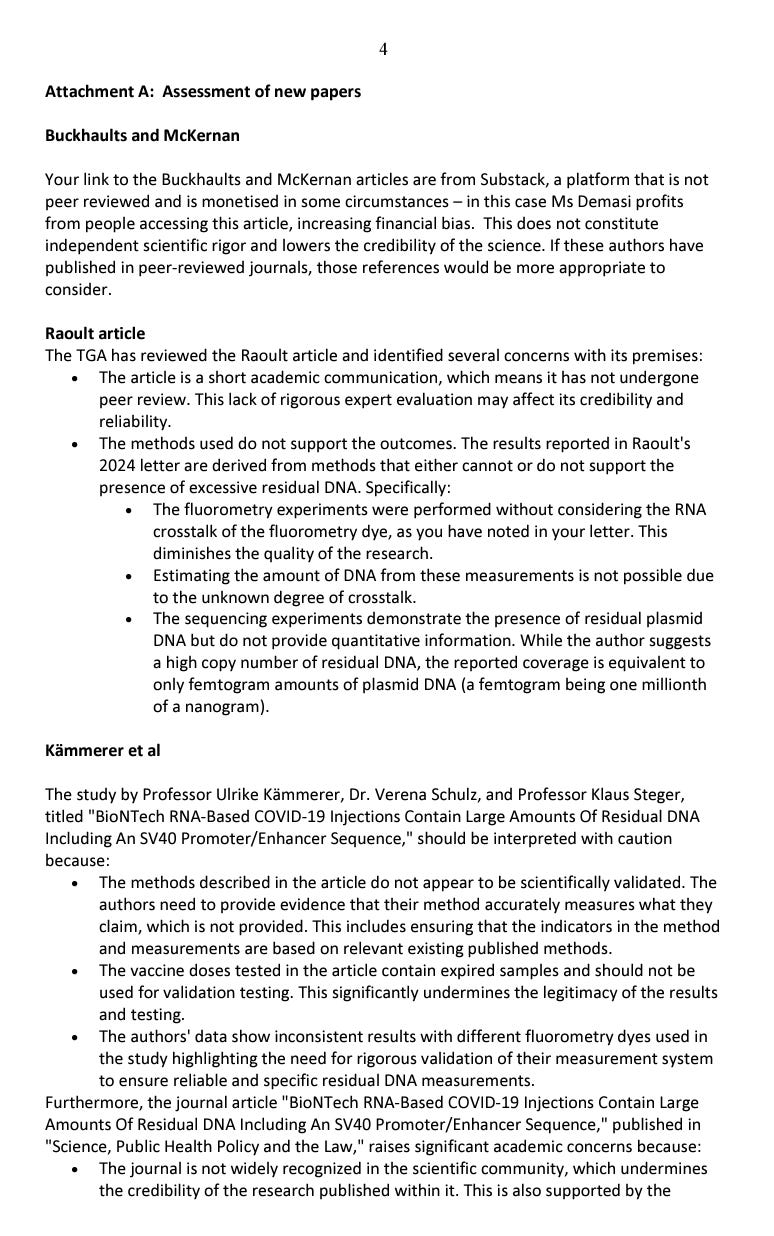
Dr. Kerr also provides an Attachment A to address recent papers that have emerged replicating McKernan et al.
She claims McKernan et al is only on Substack.
This is False.
McKernan et al is not on substack. If you don’t understand this by now, you are extremely negligent in your review of this topic.
This preprint has over 169K views and nearly 20K downloads and has now been replicated by 8 other independent labs around the world. We do not care about peer review as 50% of peer reviewed papers can’t be reproduced. This is known as the replication crisis. The below table doesn’t include Wang et al or the results of Chakraborty et al.
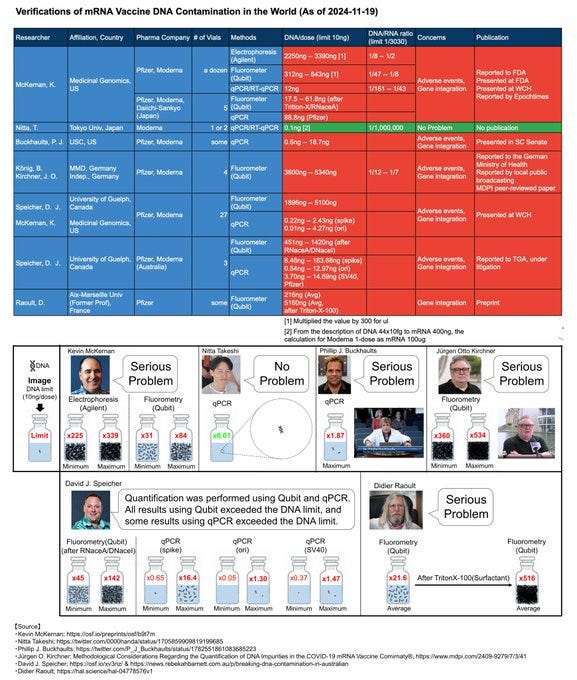
Link to Excel sheet of validating studies.
We care about transparent and independent replication. This is something our methods have achieved and Dr. Kerr’s have not.
Dr. Kerr complained that Substack is monetized. Dr. Kerr must not be aware of the peer review process. All peer reviewed journals are also monetized to a far greater extent than any substack article. “Peer review” is a $20B industry that takes most of its revenue from Pharmaceutical advertisement.
As for your comments over Raoult et al, these are addressed in Konig et al where she cites the manufacturers specifications for these assays and that the cross talk cannot inflate the values more than 5-10%. Such small inflation in signal cannot account for the log scale variance ALL labs are seeing. The use of RNaseA is ignored by Dr. Kerr?
Dr Kerr’s arguments against Kammerer et al are circular word salad. “Their methods cannot be considered validated unless they use another method which is validated” which in turn Dr. Kerr will certainly critique the other method of not being validated unless it uses another method which is validated… all while hiding your ‘validated’ method behind redactions. There is no published method that meets your ‘validation’ requirement therefore no one can question Dr. Kerr. Convenient logical fallacy Dr. Kerr has there.
Expired vials were given to patients. This argument is invalid as mentioned earlier.
Using multiple different dyes for fluorometry is good practice as it highlights the range of possible variance. This is precisely what should be done to validate an assay and now Dr. Kerr is using this thorough triple checking as a detriment of the work by Kammerer et al. Imagine if Dr. Kerr was this thorough measuring the RNA?
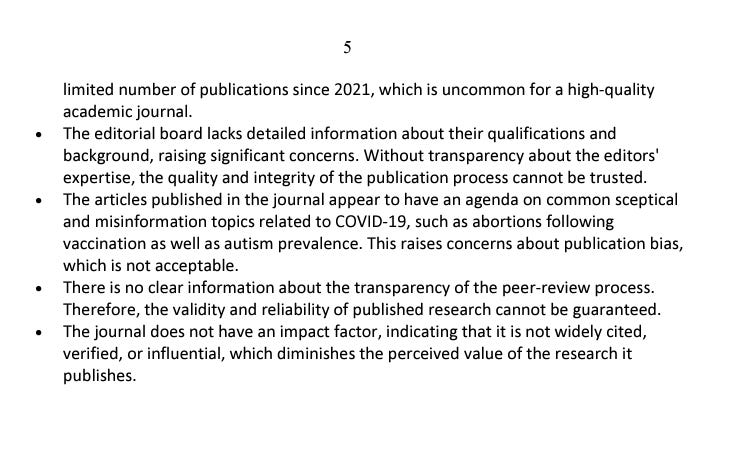
We do not engage with appeal to authority arguments over Journal reputation and citation scores. The highest impact factor journals also have the highest retraction rates.
The fact that Kammerer' et al results mirror those from McKernan, Buckhaults, Konig, Speicher, Raoult and Wang should be all that matters. But if Dr. Kerr is incapable of reading and understanding these details, I can understand how she needs to rely on reputation scores of journals to be spoon fed what to believe.
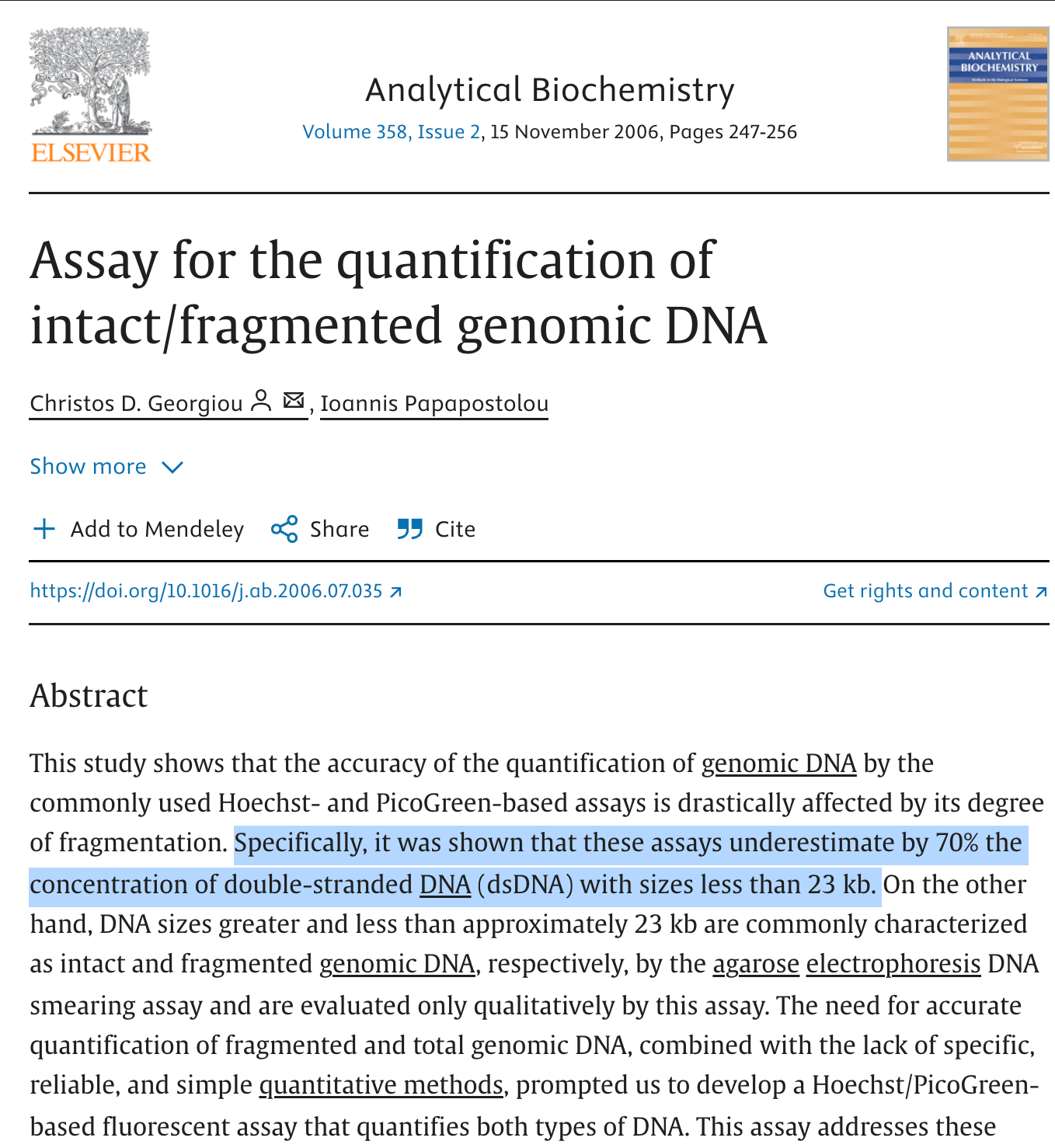
On a final note, Georgiou et al.demonstrates that PicoGreen only captures 30% of the DNA that is present once DNaseI is used to fragment the DNA so all studies to date are under measuring this problem … not overestimating it as Dr. Kerr claims without evidence.
This is Attachment A of Dr. Kerr’s letter.
Dr. Kerr states she is not aware of integration events from transfection based therapeutics. There are many things Dr. Kerr appears to be unaware of but we have provided the citations below.
These are the same tired arguments delivered from Health Canada.

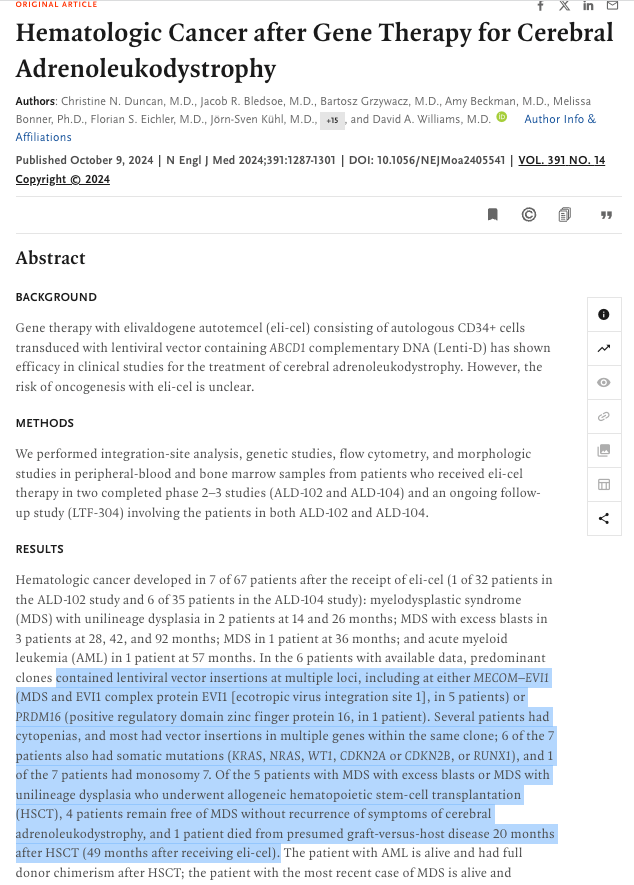
Duncan et al demonstrates 1000s of integration events using transfection of plasmids in a clinical trial. 99% of patients had an integration event. These are lentiviral plasmids which likely have a higher integration rate than SV40 based plasmids shown in Strayer et al but you cannot say you are not aware. You have now been informed.
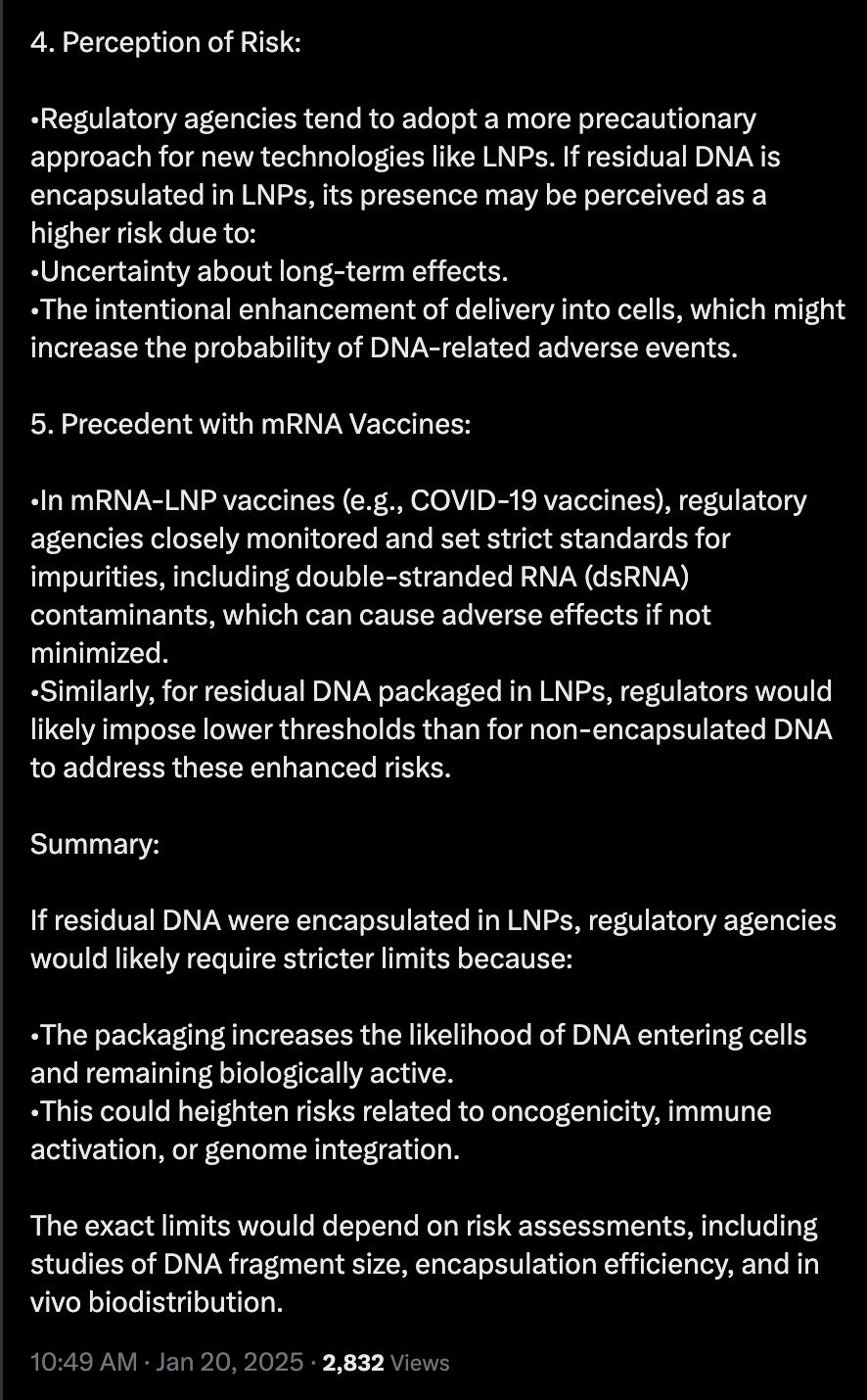
I decided to fact check Dr. Kerr’s comments with ChatGPT. It didn’t go well for her.
More details from the wonderful Vaccine Mole. Cardiac Mesothelioma after BNT162b2 injection. Mesotheliomas have been documented to be caused by SV40 virus and Asbestos exposure. Asbestos exposure increases ROS in the cell much like LNPs and Spike protein. SV40 provides the genomic instability and triggers the cGAS-STING pathway.
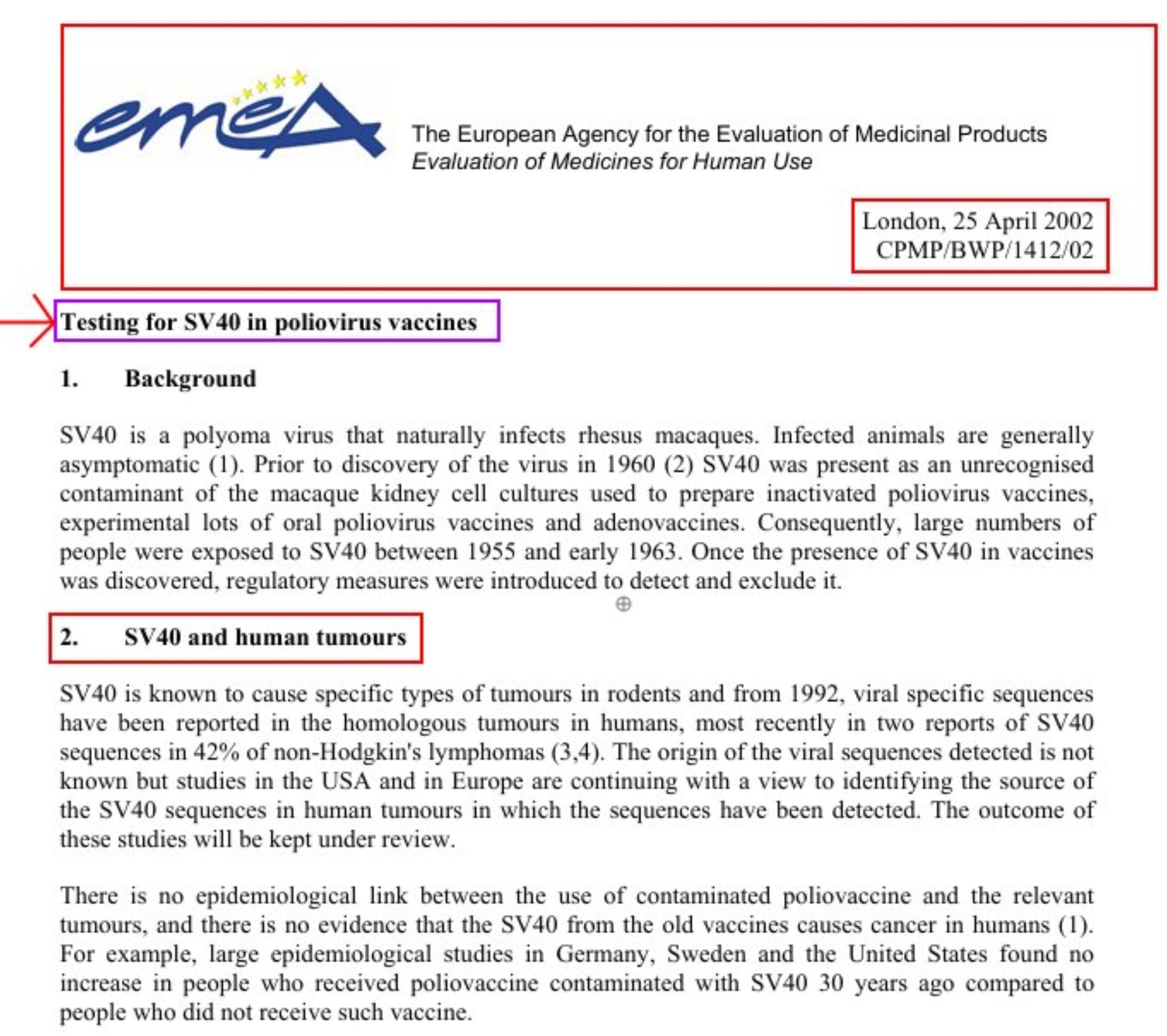
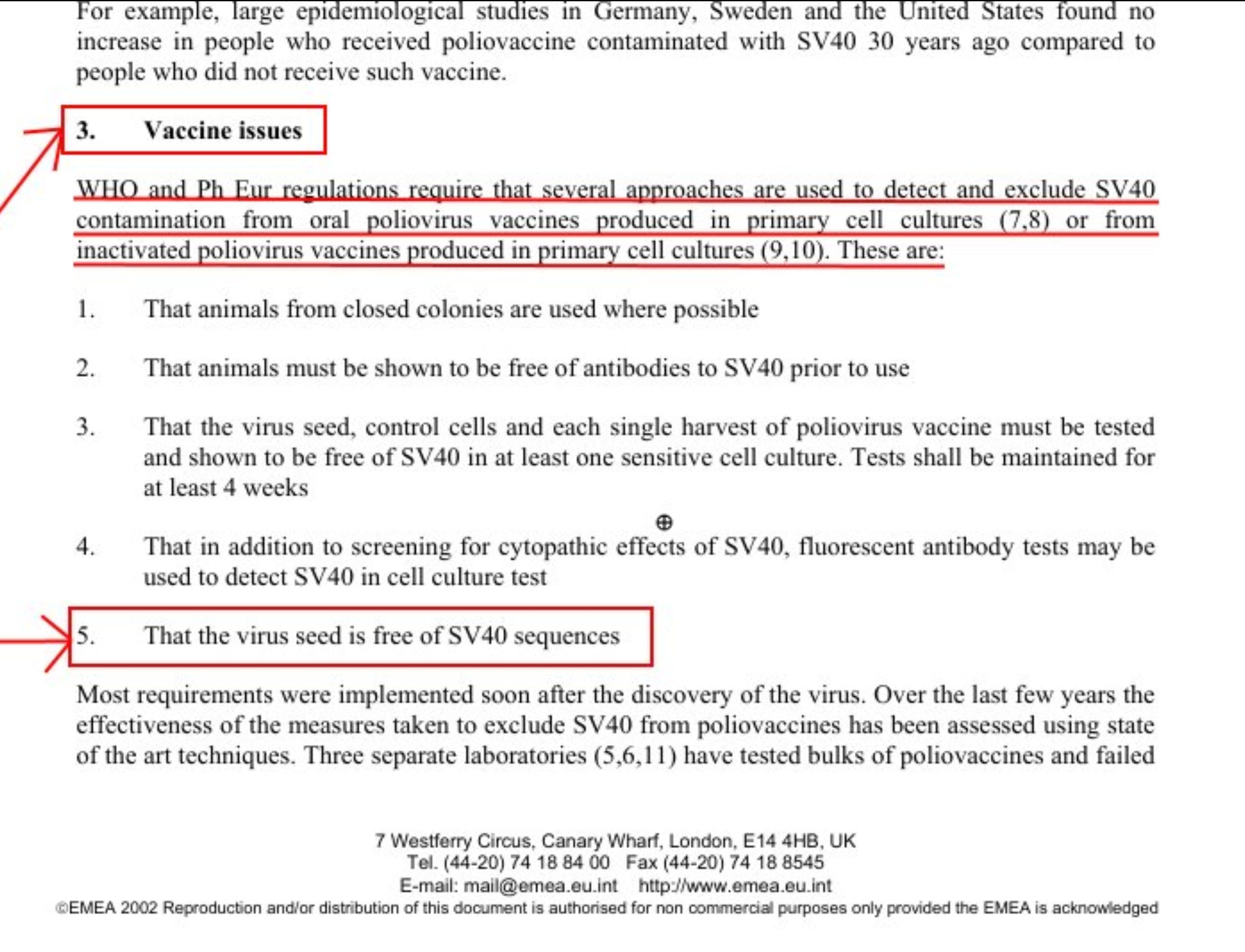
https://www.ema.europa.eu/en/testing-simian-virus-40-sv40-polio-virus-vaccines-scientific-guideline
https://www.ema.europa.eu/en/documents/scientific-guideline/testing-sv40-poliovirus-vaccines_en.pdf
In summary, Dr. Kerr’s argument can be summed up as….

Got half way through. Then I felt like I might have a stroke if I went any further. Perhaps that is the goal. If they don’t kill you with shots, they will kill you with absurdity.
I believe any questions asked of the health agencies are all passed on to pharma for pharma to answer. It must be the arrangement as health agencies know nothing scientifically about these shots and the intellectual property and all that rot. These people are just intermediaries so impossible to have a scientific exchange. Pharma has designed a very strategic plan to barricade any means of infiltration. Too bad we couldn’t invent a Trojan horse to avoid detection on our way to annihilating them. Is that too harsh? Ok, have a civilized debate.